 English
English 中文简体
中文简体 日本語
日本語 عربى
عربى русский
русский Español
EspañolNews
Xindi can provide customers with personalized, high-quality products and services to meet the needs of different markets and customers.
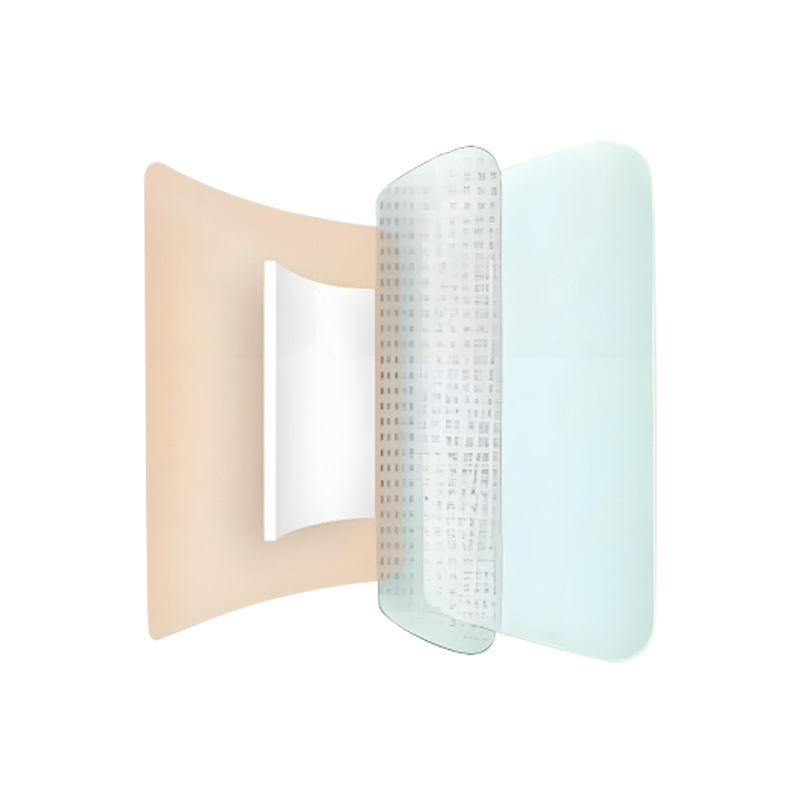
Not all wounds respond to standard dressing protocols. Patients with fragile or aging skin, chronic conditions such as diabetic ulcers or venous leg ulcers, post-surgical sites, or compromised immune systems present wound care challenges that conventional adhesive dressings often aggravate rather than resolve. The low adhesion breathable waterproof foam wound dressing patch has been engineered specifically to address these demanding scenarios — combining gentle contact layers, moisture-vapor transmission, and reliable exudate management in a single product that adapts to the patient rather than forcing the patient to adapt to the dressing.
Content
The term "low adhesion" refers to the wound-contact layer of the dressing — the surface that sits directly against the wound bed and surrounding periwound skin. In a standard adhesive foam dressing, this layer uses an acrylic or rubber-based adhesive that bonds firmly to both intact and fragile skin. For patients with normal skin integrity, this works adequately. For patients with atrophic skin, steroid-thinned epidermis, skin tears, or radiation-damaged tissue, strong adhesion creates a secondary injury at every dressing change: the adhesive strips viable tissue cells along with the dressing, causing pain, bleeding, and delayed healing.
Low adhesion foam dressings use a silicone-based or non-adherent polymer contact layer instead. Medical-grade soft silicone, the most widely used technology in this category, forms a gentle bond with dry intact skin strong enough to keep the dressing in place during normal activity, but releases cleanly from wound tissue and fragile periwound skin without trauma at removal. Clinical assessments have consistently shown that patients experience significantly lower pain scores during dressing changes with silicone-contact foam dressings compared to standard adhesive alternatives — a difference that has direct implications for patient compliance and quality of life during extended treatment courses.
The non-adherent behavior at the wound interface also prevents the dressing from incorporating into the wound bed as granulation tissue forms, which can occur with traditional gauze and some adhesive foam products. This means the dressing lifts away from the wound intact, leaving the newly formed tissue undisturbed.
Wound healing science has established since the 1960s that a moist wound environment accelerates epithelialization and reduces scar formation compared to a dry one. However, "moist" is not the same as "wet." Excessive moisture accumulation beneath a dressing — from wound exudate that cannot escape — leads to maceration, a softening and breakdown of periwound skin that enlarges the wound margin and creates a secondary site of tissue damage. Breathability, measured as moisture vapor transmission rate (MVTR), is the property that prevents this from happening.
The polyurethane foam layer in a breathable foam dressing acts as both an absorbent reservoir and a controlled moisture management system. The foam absorbs liquid exudate directly from the wound surface, locking it within its open-cell structure. Simultaneously, the backing film — a thin polyurethane membrane with a carefully engineered MVTR — allows water vapor to pass through to the atmosphere while blocking liquid, bacteria, and contaminants from entering the wound from outside. High-quality breathable foam dressings achieve MVTR values between 800 and 3,000 g/m²/24h, depending on the product grade and the exudate level it is designed for.
Selecting the correct breathability grade matters in practice. A dressing with a very high MVTR applied to a low-exudate wound may over-dry the wound bed, slowing healing. A dressing with insufficient MVTR on a heavily exuding venous ulcer will saturate quickly, leak, and cause periwound maceration. Most manufacturers offer light, moderate, and heavy exudate versions within their foam dressing ranges, with different foam thicknesses and backing film specifications. Clinicians performing wound assessments should match the dressing grade to the current exudate output and reassess regularly as healing progresses and exudate volume decreases.
The waterproof backing film that provides breathability serves a second critical function: it creates a barrier against liquid water intrusion. This property has direct practical significance for patients managing wounds in community or home care settings, where maintaining hygiene is both a clinical necessity and a quality-of-life requirement. A patient with a leg ulcer, a surgical wound, or a pressure injury who cannot bathe or shower normally faces compounding challenges — difficulty with personal hygiene, restrictions on daily activity, and the psychological burden of feeling defined by their wound.
Waterproof foam dressings allow patients to shower while wearing the dressing without compromising wound protection. The polyurethane film repels water at the surface level while continuing to allow vapor transmission outward. This bidirectional selectivity — vapor out, liquid in blocked — is a specific property of the film structure and is not simply achieved by applying any waterproof material. Clinicians and patients should confirm that a dressing labeled "waterproof" has been validated for showering in its product documentation, as the degree of water resistance varies between products.
For pediatric patients, elderly patients in assisted living environments, or athletes recovering from minor wounds, the ability to maintain normal hygiene and participate in rehabilitative activities without constant dressing changes is a meaningful improvement in care experience. Fewer dressing changes also reduce overall care costs and the cumulative trauma to periwound skin from repeated adhesive application and removal.
The combination of low adhesion, breathability, and waterproofing makes this dressing category particularly well suited to several patient groups whose wound care needs exceed what standard products can reliably provide.
Aging skin loses dermal collagen, subcutaneous fat, and epidermal thickness, making it highly vulnerable to adhesive-related injury. Medical adhesive-related skin injury (MARSI) is a recognized clinical problem in geriatric care, encompassing skin tears, tension blisters, contact dermatitis, and folliculitis caused by repeated dressing application. Low adhesion silicone foam dressings are now recommended as a first-line product for this population by multiple wound care associations, including the European Wound Management Association (EWMA), precisely because they reduce MARSI risk while maintaining reliable wound coverage.
Diabetic foot ulcers require precise moisture management, protection from external contamination, and atraumatic dressing changes — often over many months of treatment. The periwound skin in diabetic patients is frequently compromised by neuropathy, poor circulation, and prior tissue damage. A low adhesion foam dressing applied to a diabetic plantar ulcer maintains the moist wound environment needed for granulation, protects against bacterial ingress, and allows inspection and dressing change without causing new tissue injury. The cushioning property of the foam layer also provides a degree of pressure redistribution over the wound site during ambulation.
Surgical incisions and procedural wounds, including biopsy sites, graft donor areas, and skin cancer excision margins, benefit from breathable waterproof coverage during the initial healing phase. The waterproof backing allows normal hygiene without dressing compromise, while the low adhesion contact layer protects the delicate wound edges from tension and trauma during the first critical days of epithelialization. For patients who have undergone skin grafts, non-adherent foam dressings are particularly important because any mechanical disruption to the fragile new graft can cause graft failure.
Neonatal skin, especially in premature infants, has a poorly developed stratum corneum that offers minimal resistance to adhesive-related injury. Even moderate adhesives can strip the epidermis of a preterm neonate, creating wounds that become portals for infection in an already immunocompromised patient. Silicone-based low adhesion foam dressings sized and shaped for neonatal and pediatric applications provide the gentlest possible wound coverage option for this vulnerable population, and their use is supported by neonatal intensive care unit (NICU) clinical guidelines in multiple countries.
The table below summarizes how low adhesion breathable waterproof foam dressings compare with common alternatives across the performance parameters most relevant to special care applications.
| Dressing Type | Atraumatic Removal | Moisture Management | Waterproof | Suitable for Fragile Skin |
|---|---|---|---|---|
| Low Adhesion Breathable Waterproof Foam | Excellent | Excellent | Yes | Yes |
| Standard Adhesive Foam | Moderate | Good | Varies | Limited |
| Hydrocolloid Dressing | Poor–Moderate | Moderate | Yes | No |
| Paraffin Gauze | Good | Poor | No | Moderate |
| Alginate Dressing | Good (when moist) | High absorption only | No | Moderate |
To achieve the full benefit of a low adhesion breathable waterproof foam dressing, correct application and removal technique is essential. Even a well-designed product can cause harm if handled incorrectly.
The low adhesion breathable waterproof foam wound dressing patch represents a clinically significant advancement for patients whose care requirements exceed what conventional wound products can safely meet. By eliminating adhesive trauma, actively managing moisture balance, and enabling normal daily hygiene, it removes three of the most common barriers to smooth, complication-free wound healing — making it an essential product in any serious wound care formulary.
 Absorbent, Moisturizing And Non-Irritating Hydrocolloid Acne Patch
Absorbent, Moisturizing And Non-Irritating Hydrocolloid Acne Patch
 Cushioning, Pressure Reducing, Breathable And Comfortable Heel Patch
Cushioning, Pressure Reducing, Breathable And Comfortable Heel Patch
 Soft Waterproof and Odor Control Ostomy Pouch
Soft Waterproof and Odor Control Ostomy Pouch
 Widely Used Waterproof And Dustproof Silicone Scar Sheets
Widely Used Waterproof And Dustproof Silicone Scar Sheets
 Hypoallergenic Breathable Waterproof Ear Patches
Hypoallergenic Breathable Waterproof Ear Patches
 Strong Adhesive And Drug-Free Anti-Snoring Patch
Strong Adhesive And Drug-Free Anti-Snoring Patch
 Long-Lasting Mosquito Repellent, Safe And Gentle Mosquito Repellent Stickers
Long-Lasting Mosquito Repellent, Safe And Gentle Mosquito Repellent Stickers
 Soothing And Anti-Itching, Mild And Hypoallergenic Soothing Sticker
Soothing And Anti-Itching, Mild And Hypoallergenic Soothing Sticker
 Invisible Non-Slip And Sweat-Proof Nipple Covers
Invisible Non-Slip And Sweat-Proof Nipple Covers
 Portable Design And Reusable Ventilation Nose Strips
Portable Design And Reusable Ventilation Nose Strips
 Breathable Comfort Fit Swimming Private Patches
Breathable Comfort Fit Swimming Private Patches
 Strong Adhesion Waterproof And Sweatproof Anti-Exposure Stickers
Strong Adhesion Waterproof And Sweatproof Anti-Exposure Stickers
Copyright © 2024 by Wuxi Xindi Medical Technology Co., Ltd. All Rights Reserved.
medical adhesive tapes manufacturers